- Visibility 41 Views
- Downloads 11 Downloads
- DOI 10.18231/j.adr.2024.020
-
CrossMark

Radicular cyst: A rare case report
- Author Details:
-
 Rohan Shil
Rohan Shil
-
Rahul Shil *
Introduction
Radicular cysts can also be referred to as apical periodontal cysts, dental cysts, periapical cysts, or root-end cysts. It is one of the most prevalent jaw cysts, accounting for 52–68% of the overall cysts found in the mandible.[1] The reason for this cyst's development is the inflammation of the epithelial ligament in the periodontal ligament.[2] The radicular cyst pathogenesis described three phases for its occurrence, such as the phase of initiation, cyst formation, and enlargement.[3], [4] Acute exacerbations of cysts, which are characterized by pain, redness, swelling, and pus discharge, are occasionally caused by long-standing lesions; however, these cases are rarely detected until they are identified by routine radiology assessment.[5] It is non-keratinized stratified squamous epithelial layer (6 –100 layers) lining with an arcading pattern.
Case Description
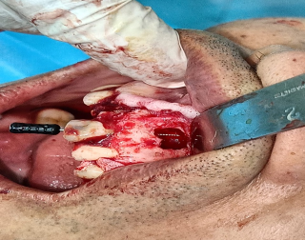
A 55-year-old male patient reported to dent mate dental clinic with a primary complaint of pain in the maxillary anterior region. Further examination confirmed that there was a deep cavity in the 23 region (TOP +ve) and a discolored tooth restored with composite filling in the 21 regions. We have decided to take an IOPA X-ray. After taking the IOPA X-ray, we found that there is a well-defined radiolucency involving the periapical region of 21. A well-defined sclerotic border was present around 21. After further questioning, the patient confirmed the history of swelling and pus discharge a few years ago. The routine blood examination report was normal. On the basis of the radiological and clinical results, a periapical cyst of 21 was diagnosed. A negative response to electric and thermal pulp vitality testing was noted on 21 when the adjacent tooth showed a normal response. Teeth were not tender to vertical percussion. The treatment for 21 was RCT (root canal treatment), followed by enucleation and apicectomy. For which consent was obtained from the patient. A single-sitting RCT was carried out following surgical cyst enucleation and apicectomy. On cyst enucleation, lignocaine with 2% adrenaline was given to anesthetize the area. The mucoperiosteal flap was elevated, and the bony overlying the cyst was removed. Cysts were removed from the bony cavity using a spoon-type curette. Furthermore, apicectomy was done by using a round bur and obturating the tooth using gutta-percha. Flap closure was also done using a 3.0 silk suture. A specimen was sent for histopathology examination, which confirmed the radicular cyst.



Discussion
A cyst is a pathological cavity that is not formed by the buildup of pus but has a fluid, semi-fluid, or gaseous substance.[6] Cysts can occur within the bone or soft tissues. Radicular cysts have been classified as inflammatory because, in the majority of cases, they are the consequences of pulpal necrosis following caries.[7] Radicular cysts are one of the most frequently seen jaw cysts in the oral and maxillofacial regions, especially around the incisors and canines. The cyst slowly increases in size to eventually cause cortical plate expansion, which is characterized by eggshell crackling.[8] It is less common in deciduous teeth as compared to permanent teeth. Histologically, it is a non-keratinized stratified squamous epithelial lining with an arcading pattern, Rushton bodies, a connected tissue wall with inflammatory cells, and cholesterol clefts. A radicular cyst can be managed by non-surgical endodontic treatment like RCT, but in some cases, surgical management might be needed for a better prognosis. A follow-up is important in such cases.
Conclusion
Although radicular cysts are a very frequent condition in the oral cavity, they are typically not observed on time. Depending on where and how big the cysts are, there are now a variety of therapeutic options. Large cysts can be treated endodontically, followed by enucleation. Furthermore, many dentists advise non-surgical therapy for minor lesions, while there is now debate over the best course of action. Treating physicians must therefore possess the necessary knowledge to handle such cases at different stages. The authors also believe that by providing this case report, novice dental surgeons will be better able to handle similar occurrences.
Source of Funding
None.
Conflicts of Interest
There is no conflicts of interest reported in this study.
References
- L Govindaraju, DP Antony. Surgical Management of Radicular Cyst With the Application of a Natural Platelet Concentrate: A Case Report. Cureus 2023. [Google Scholar]
- L Bodner. Cystic lesions f the jaws in children. Int J Pediatr Otorhinol 2001. [Google Scholar]
- . Evaluation of P63 Expression in Keratocystic Odontogenic Tumor, Dentigerous Cyst and Radicular Cyst- An Immunohistochemical Study - ProQuest. . [Google Scholar]
- SM Balaji, PP Balaji. . Textbook of Oral & Maxillofacial Surgery - E Book 2018. [Google Scholar]
- . Jaw tumors and cysts - Symptoms and causes - Mayo Clinic. . [Google Scholar]
- J Seehra, K Horner, P Sloan. The Unusual Cyst: Solitary Bone Cyst of the Jaws.. Dental Update 2009. [Google Scholar]
- B Kumar, S Shroff. Management of an Infected Maxillary Periapical (Radicular) Cyst through Nasal Antrostomy. J Health Sci Res 2016. [Google Scholar]
- S Karpagavalli, S Subramanian, V Vaishnavi, G Sivadas. Bilateral Radicular Cyst - A Rare Case Presentation. SADJ 2022. [Google Scholar]